Radial-Sided Wrist Pain: The Scapholunate Ligament Injury
What is it?
The scaphoid and the lunate are 2 very important carpal bones sitting atop the distal end of the radius bone (Figure 1). This forms part of the essential articulation in the wrist joint. Strong ligaments between the carpal bones (intercarpal ligaments) hold these components together. These ligaments are strong enough to withstand an axial load placed across the wrist joint without giving way, whilst being flexible enough to allow range of motion between the carpal bones to enable smooth movements in the wrist joint. The ligament between the scaphoid and the lunate bone, known as the scapholunate ligament, is the most commonly injured of all the intercarpal ligaments. In a complete tear, the connection between the scaphoid and the lunate is lost, and it is termed scapholunate dissociation (Figure 2). This upsets the balance in the wrist joint and results in asynchronous and uncoordinated motion between the carpal bones during wrist movement. This may cause pain, swelling, clicking, loss of grip strength and loss of range of motion in the wrist joint. In longstanding cases, a condition called scapholunate advanced collapse (SLAC) can develop. The late stages of SLAC are irreversible and result ultimately in unsalvageable osteoarthritis of the wrist joint.
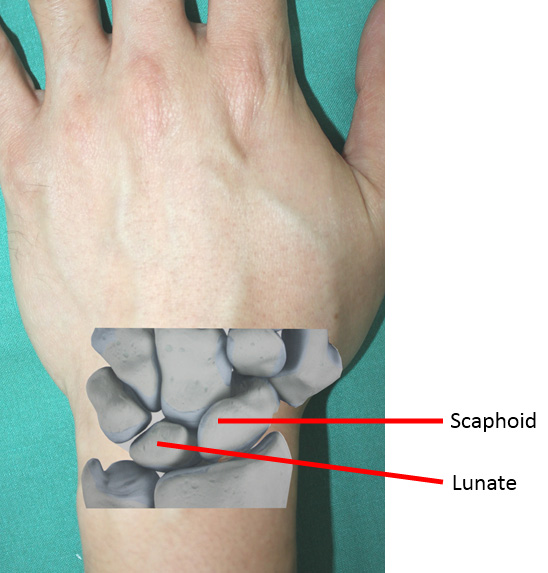
Figure 1. Picture showing the
scaphoid and lunate in the wrist.

Figure 2. An X-ray showing scapholunate
dissociation (indicated by arrows).
How does the injury occur?
The scapholunate ligament injury occurs in axial overloading of the hyperextended wrist joint. This most commonly occurs in a fall with an outstretched hand. The energy is absorbed by the scapholunate joint and can result in a sprain, partial tear or complete tear of the scapholunate ligament (Figure 3). In the elderly or osteoporotic person, such a fall usually results in a wrist fracture and the scapholunate ligament may or may not be affected in these cases. In recent studies, it has also been discovered that the scapholunate ligament is injured concomitantly in patients with fractures of the wrist. The scapholunate ligament injury in these cases is commonly overlooked.
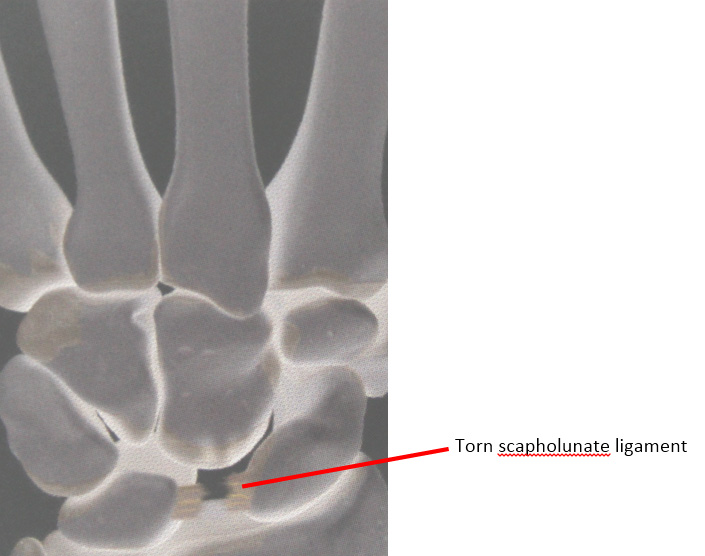
Figure 3. Complete tear of the scapholunate
ligament, giving rise to scapholunate dissociation.
How do I know if I have a scapholunate ligament injury?
In the absence of any fracture, pain and swelling over the dorso-radial aspect of the wrist which persist despite adequate rest and immobilization are key symptoms which may suggest the presence of this injury. A consultation with a qualified Hand Surgeon is essential. During the consultation, a detailed history will be taken. Clinical examination of the affected wrist will reveal tenderness over the dorsal aspect of the scapholunate joint. Dynamic stress tests, such as the Watson shift test, will enable the Hand Surgeon to clinch the diagnosis. Plain radiographs of both wrists in specific clenched fist views will help to determine the presence and severity of the dissociation between the scaphoid and the lunate bones. Finally, a magnetic resonance imaging (MRI) scan of the affect wrist may be necessary to distinguish between a sprain and a partial tear of the scapholunate ligaments.
What are the treatment options?
In cases of scapholunate ligament sprain or minor tears, non-surgical management involves rest immobilization of the wrist in a custom-molded thermoplastic splint for a period of 6 weeks. Hand therapist-guided rehabilitation is then commenced after this 6-week period. Additionally, non-steroidal anti-inflammatory medications are prescribed to reduce pain and inflammation resulting from the injury.
If this treatment modality fails to resolve the symptoms, arthroscopic wrist surgery may be indicated. Exploration and debridement of inflammatory tissue around the scapholunate joint, followed by thermal shrinkage of the injured scapholunate ligament using a radiofrequency probe is then performed. Post-operatively, the wrist is again immobilized and rested for 6 weeks before rehabilitation is started with the hand therapist.
In complete scapholunate ligament tears resulting in scapholunate dissociation, rotatory subluxation of the scaphoid and carpal collapse before the onset of osteoarthritis, surgical reconstruction of the scapholunate ligament is indicated.
Reconstruction of both the dorsal and volar aspects of the scapholunate ligament truly replicates normal anatomy and closely restores normal biomechanics in the scapholunate joint. This surgery is done as a Day Surgery procedure under general anaesthesia. It involves harvesting part of the flexor carpi radialis tendon and using this strip of tendon to reconstruct the scapholunate ligament by passing it through multiple bone tunnels drilled into the scaphoid and lunate bones before securing it with strong sutures to the dorsal wrist capsule (Figure 4).
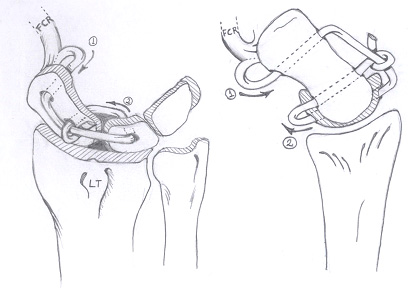
Figure 4. Pictorial diagrams of volar and dorsal scapholunate ligament
reconstruction using a partial flexor carpi ulnaris tendon graft.
Why see a Hand Surgeon for a scapholunate injury?
A Hand Surgeon is the best qualified specialist doctor to diagnose and manage the entire spectrum of this injury. Scapholunate reconstruction is a complex surgical procedure requiring precise handling of both soft tissue and bony structures to produce the best results and this is best delivered by a Hand Surgeon. Hand Surgery centres with dedicated hand therapists who work hand-in-hand with the surgeons will give an additional advantage in patients’ recovery. Constant feedback between the patient, doctor and hand therapist allows for a bespoke rehabilitation process and optimized outcome.